
This guide is a work in progress. It will be updated as the journey continues.
 Introduction
Introduction
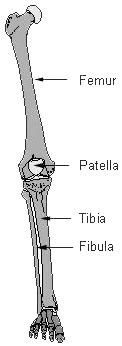
A normal human leg consists of a femur in the upper leg connected to the hip and a lower leg consisting of a tibia and a smaller fibula connecting to the small bones in the foot. Joining these is a knee joint with a patella bone.
Tibial Hemimelia (Missing or underdeveloped tibia) and the similar Fibular Hemimelia (Missing or underdeveloped fibula) are birth defects in the bones of the lower leg. The patella may be missing. The foot may have missing or deformed bones and toes. The foot is almost always flipped up.
My daughter Lulu was born with Tibial Hemimelia (TH), so rare a condition that it is present in only one-in-a-million live births. Compare this with Down Syndrome at approximately one-in-a-thousand. Even rarer at one-in-three-million is the bilateral (affecting both legs) form. She could not walk. Instead, she moved around on her knees.

Diagnosis
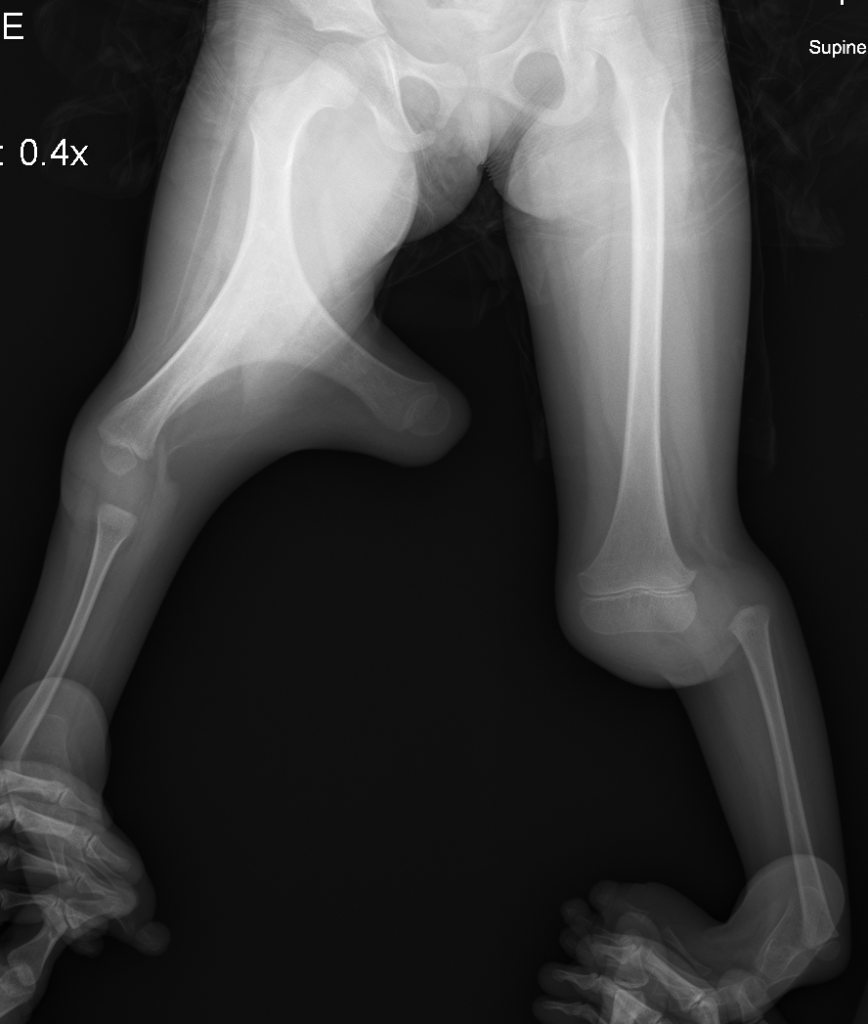
Lulu’s condition was caused by Gollop-Wolfgang syndrome, an ultra-rare genetic condition. She was diagnosed with TH Type 5A on her left leg and Type 5Bi on her right leg, among the worst deformities on the Paley classification chart. She also had a forked right femur with two intact condyles. Notice the absence of a tibia in the X-Ray:
TH and FH differ on a spectrum of severity by what is missing and what is not. The potential treatment options and outcomes vary accordingly. The near-universal treatment for these conditions is amputation of the lower leg at the knee followed by lifetime prosthetic use. Dr. Dror Paley is one of the few doctors who opt for limb salvage and reconstruction and is by far the leading expert in the field, having pioneered or enhanced many treatment approaches. Even some of his critics acknowledge his expertise.¹
Treatment
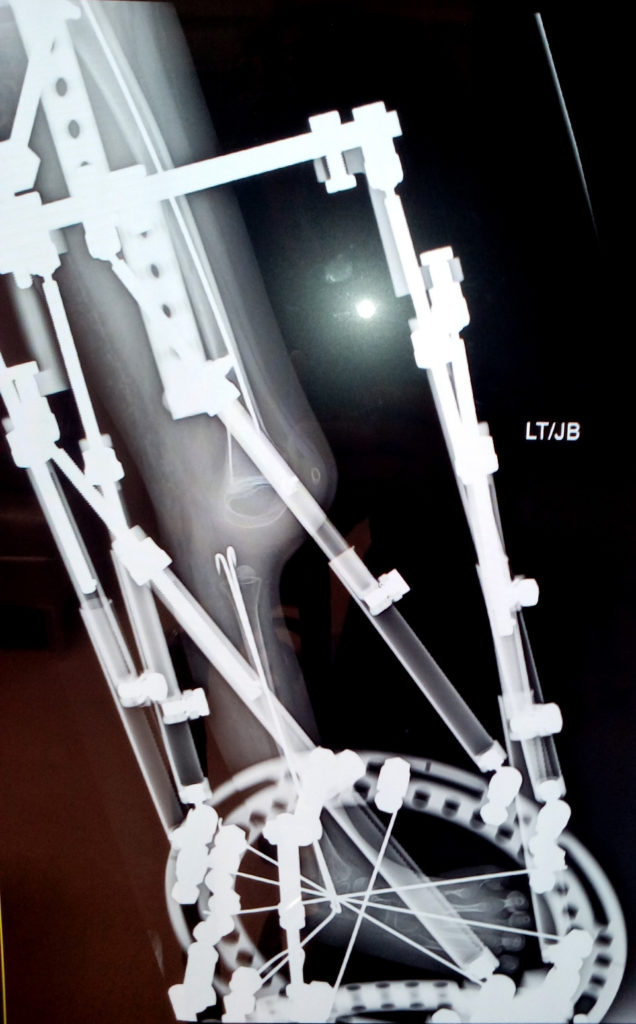
Lulu had her left leg placed in an external fixator. The fixator is used to move the fibula into the position where the tibia would have been. With the fixator on, the fibula can move up to 1mm per day. This slow movement allows the soft tissues to stretch and heal without damaging them.
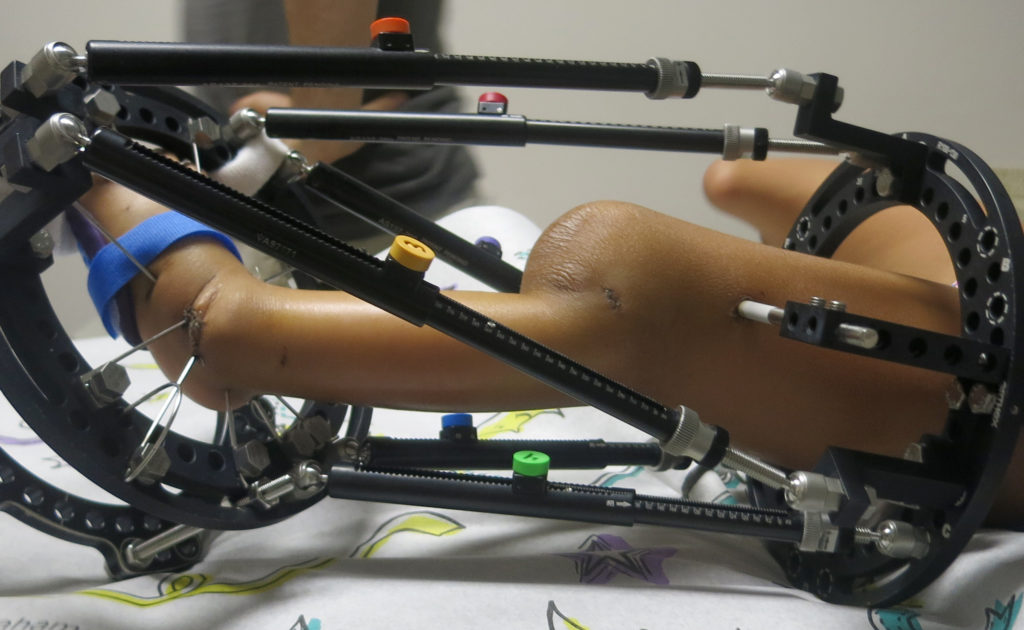
Once the fibula is in position, it will be used as a replacement tibia. The patella will be cut into two pieces. The smaller piece will be left behind to grow a new one. The larger piece will be flipped and fused to the top of the fibula, forming a superior bone ending. A knee (re)construction is then performed to make a functioning knee.
Her right leg lacked a proper quadriceps to provide a sufficiently functional knee joint so we were forced to choose amputation. The Y-shaped femur was cut and the two condyles brought together to form a larger bone base. The purpose is twofold: straighten the leg and provide a better fit for the prosthetic.

At this stage of treatment she is able to walk by herself on her fixator using a reverse walker. It is the first time she has ever been able to walk unassisted by another person.
After a number of weeks of healing, she was allowed to bear weight on her stump. She was fitted for a prosthetic and able to walk on two feet for the first time:
(more to come)
Bibliography
- Pediatric Lower Limb Deformities. Chapter 24: Tibial Hemimelia. Dror Paley and David Y. Chong. Springer.
- Treatment Strategies for Tibial Hemimelia. Dr. Dror Paley. The Paley Institute (2016).
- The Knee Disarticulation. Douglas G. Smith, MD (2004)
¹ It is still considered controversial in polite society to suggest that the default treatment for FH and TH should be to attempt limb salvage, rather than amputation. Few doctors will even mention any other possibility. In these cases fully informed consent only happens for those who do their own research. Making this suggestion will result in statements about how great prosthetics are, bans from topical groups and forums, hateful comments, and other similar bad behavior. As such Dr. Paley, as well as those who advocate for limb salvage, will take heat for trying to avoid amputation.
Please see the Treatment Options for Tibial Hemimelia for more information on the decision making factors.
Dear Mr. Ramsey,
I just wanted to take a moment to tell you how amazed and grateful I am for what God has done for your family. Hearing about Lulu and how God worked a miracle in preserving her ability to walk truly moved me. It’s incredible to see such a clear reminder of His power, care, and faithfulness.
Before this, I had never even heard of TH, and learning about it gave me a deeper appreciation for how serious and challenging it can be. Knowing that, the outcome makes God’s work in Lulu’s life even more remarkable. I’m genuinely thankful and rejoicing with you and your family.
I also wanted to mention that I know your son Avery, and it felt important to reach out and let you know how encouraged I am by your family’s story.
Thank you for being willing to share such a meaningful testimony.
Sincerely,
Micah Peirce
Micah,
Thank you. I really appreciate your kind words.
Peace,
DR